Overview of Lyme Borreliosis (A Bioregulatory Medicine Approach)
by: James Odell, OMD, ND, L.Ac., BRMI Medical Director
The information in this monograph is intended to help users better understand current diagnostic and bioregulatory medicine treatment protocols related to tick-borne illnesses. Information is based on review of scientific research data, historical practice patterns, and clinical experience. This information should not be interpreted as specific medical advice. The management of tick-borne illnesses in any given patient must be approached on an individual basis using the practitioner’s best judgment. Users should seek the advice of a physician before using any protocol listed in this monograph. The protocols raise many issues that are subject to change as new data emerge. The reader assumes the risk of any injuries. None of the suggested protocol regimens can guarantee health benefits. Users should consult with a qualified healthcare provider for specific questions regarding therapies, diagnosis and/or health conditions, prior to making therapeutic decisions.
———————
Lyme disease, also called Borreliosis, might be the most insidious and least understood of infectious diseases of our day. Lyme disease is an infection that is caused by different genospecies of the Borrelia bacteria and primarily transmitted by the bite of an infected tick. According to Center for Disease Control (CDC) reports, Lyme disease caused by Borrelia is currently the most common vector-borne disease in the United States.1 There are several species, subspecies and strains of this bacteria. This great diversity of species and strains contributes to its ability to evade the immune system and antibiotic therapy, thus leading to a chronic infection (post-treatment Lyme disease syndrome or PTLDS). PTLDS is often associated with neurological symptoms that are both debilitating and increasingly difficult to treat with conventional antibiotics.2 The Borrelia spirochete has developed numerous adaptive features that makes it unique among pathogenic bacteria and thus can lead to PTLDS.3
Borrelia‘s Adaptive Features
Borrelia‘s adaptive features ensure its survival and confer resistance to antibiotics. Borrelia, like the bacteria that causes syphilis, is a spirochete. Spirochetes are a group of bacteria that have a unique mode of motility by means of axial filaments called endoflagella. When these filaments rotate, the spirochetes move in cork-screw fashion. This type of movement is thought to be an adaptation to viscous environments, such as aquatic sediments, biofilms, mucosal tissues, collagen tissue and the intestinal tracts of animals. This feature allows the spirochetes to hide their flagella from the host immune defenses. Borrelia‘s membrane has a composition like the cells of mammals in that it contains phosphatidylcholine (PC), a type of phospholipid. Phospholipids are a class of lipids or fats that are a major component of all cell membranes. Because our nervous system is rich in PC, the spirochete tends to associate itself with our nervous system as a source of PC for its membrane. Hence, it feeds on us. It has also been suggested that having a cell membrane high in PC, and therefore “looking” like one of our own cells, may aid Borrelia in its effort to avoid our immune system.4
Borrelia has one of the most advanced and complex DNA structures of any bacteria known. This allows it to assess its surrounding chemistry and alter its cell membrane to ensure its survival. Thus, Borrelia is the ultimate escape artist. It can invade a variety of cells, including endothelium, fibroblasts, lymphocytes, macrophages, keratinocytes, synovium, and most recently neuronal and glial cells. By “hiding” inside these cells, the spirochete can evade the immune system and be protected to varying degrees against white cells and antibiotics, allowing the infection to persist.5
The spirochete can change its form to rounded forms, sometimes called spheroplasts, which either lack a cell wall or have a damaged cell wall.6 This too is a survival technique that can protect it from antibiotics. Data suggest these rounded cells are virulent and infectious, can survive under adverse environmental conditions, and may revert to the spiral form, once conditions are more favorable. Antibiotics are ineffective against these spheroplasts.7, 8, 9
Stages and Manifestations of Lyme Borreliosis
The disease is described as having three stages: early localized, early disseminated and late disseminated. However, the stages can overlap and not all patients go through all three. A bull’s-eye rash is usually considered one of the first signs of infection, but many people develop a different kind of rash or none at all. The last stage, because of domination of neurologic symptomatology, is called “neuroborreliosis”. The brain has a highly selective permeable barrier called the blood-brain barrier that normally protects the brain from foreign invaders. However, Borrelia‘s unique characteristics allow it to penetrate this protective barrier. Thus, neurological symptoms are present with chronic Lyme disease because Borrelia and its endotoxins (neurotoxins) infect the brain and central nervous system causing inflammation and various neurological symptoms such as pain, headaches, tremors, seizures, and brain fog.10
It has been said that the longer one is ill with Lyme the more endotoxin/neurotoxin is present in the body. It probably is stored in fatty tissues, and once present, persists for a very long time. This may be because of enterohepatic circulation, where the toxin is excreted via the bile into the intestinal tract, but then is reabsorbed from the intestinal tract back into the blood stream.
Mainstream infectious disease doctors argue that there is no evidence that Lyme borreliosis remains in the body after a few weeks to a month of antibiotic treatment. The laundry list of symptoms in patients may be persistent, but these conventional doctors claim that it is not due to a chronic Lyme infection. On the other side, many doctors that specialize in Lyme disease blame Borrelia and coinfections for triggering chronic neurological and psychiatric symptoms.
A comprehensive therapeutic bioregulatory medicine approach considers the stage as well as the individual’s unique constitution and the biological terrain that is affected.
Spirochetes have an affinity for connective tissue. The following are 5 tissues that are commonly infected:
- ligaments and joints (asymmetric affliction of large joints, especially hip and knee)
- skin and subcutaneous tissues (collagen breakdown and premature aging)
- meninges and astroglia (connective tissue of brain)
- heart tissue
- aqueous humor of the eye
Symptoms
Borrelia spirochete releases bacterial lipoproteins (BLP) which cause numerous symptoms. The following is a checklist of common symptoms seen in various stages of Lyme disease:
Localized Early (Acute) Stage:
- Solid red or bull’s-eye rash, usually at site of bite
- Swelling of lymph glands near tick bite
- Generalized achiness
- Headache
Early Disseminated Stage:
- Two or more rashes not at site of bite
- Migrating pains in joints/tendons
- Headache
- Stiff, aching neck
- Facial palsy (facial paralysis like Bell’s palsy)
- Tingling or numbness in extremities
- Multiple enlarged lymph glands
- Abnormal pulse
- Sore throat
- Changes in vision
- Fever of 100 to 102 F
- Severe fatigue
Late Stage:
- Arthritis (pain/swelling) of one or two large joints
- Disabling neurological disorders (disorientation; confusion; dizziness; short-term memory loss; inability to concentrate, finish sentences or follow conversations; mental “fog”)
- Numbness in arms/hands or legs/feet
Basic Bioregulatory Medicine Approaches for Lyme and its Co-infections
The goals in treating Lyme disease are to eliminate the Borrelia infection, to resolve symptoms and return patients to their prior quality of life, and to prevent patients from experiencing recurrent episodes from an untreated or inadequately treated infection.
There are at least five basic guiding principles used to achieve this goal.
- Decrease pathogenic microbial load
- Improve the intestinal and oral microbiome
- Decrease total toxic body burden
- Balance and modulate the immune system, thereby improving the bodies’ natural defenses and reducing inflammation
- Improve bioregulatory mechanisms (heme synthesis and methylation) with supplementation
To achieve this, it is necessary to utilize a comprehensive multitherapeutic approach in the treatment of Lyme and its coinfections. The following list (though far from complete) describes therapies used towards these principles:
- Identify food allergens and eliminate those foods. Diets that are pro-inflammatory and depleted of nutrients (i.e., the average American diet) cause imbalances in the body’s biochemistry. Specifically, the body will become more acidic and inflamed, and less oxygen will be available on the cellular level. Consider a low lectin11, anti-inflammatory diet as described in The Plant Paradox by Steven Gundry, MD.
- Decrease microbial load using plant-based antimicrobials, IV ozone therapy and ozonated rizols (Biopure). There are several herbs that have been clinically used to treat Lyme and its co-infections. Some are used solo, some work better in combination, and there are many specific formulations available as well. This, as all therapy, needs to be individually assessed as to dosage, timing and herbal alterations or rotations. An excellent text on plant-based antimicrobials is Healing Lyme by Stephen Buhner – http://buhnerhealinglyme.com/ (see APPENDIUM 1)
- Identify and supplement nutritional deficiencies
- Improve errors in heme synthesis. Heme is an iron-containing molecule that occurs naturally in every single plant and animal. It is an essential molecular building block of life and gives the blood its ability to carry oxygen. Kryptopyrroluria, also called hemopyrrollactamuria (HPU), is a metabolic disorder disrupting heme synthesis. This disorder results in a significant loss of zinc, vitamin B6, biotin, manganese, and other important nutrients from the body via the kidneys. It has been proposed that the incidence of HPU in Lyme disease may be 80% or higher, particularly in patients with toxic element excess (lead, mercury, cadmium, and others).12, 13 Thus, patients with symptoms of chronic Lyme disease might benefit from kryptopyrrole testing, and if positive, a supplemental treatment protocol that addresses nutritional deficiencies.14
- Detoxify environmental toxins – these can make Borrelia more virulent and difficult to treat. Decrease the total toxic body-burden (toxic element excess) by activating organs of detoxification – liver, spleen, intestine, lung, kidneys and skin. There are several nutrients, such as chlorella and cilantro, that help facilitate toxic element removal. Sauna is also very helpful.
- Get enough sleep; practice sleep hygiene – EMF and WIFI Free Sleep
- Improve lymphatic circulation – Lymph massage, dry brushing, and colon hydrotherapy.
- Minimize Herxheimer reactions when using antimicrobials. A ‘Jarisch–Herxheimer reaction’ is a body reaction to endotoxin-like products released by the death of harmful microorganisms within the body, usually during antibiotic treatment. Antimicrobial therapy results in lysis (destruction) of bacterial cell membranes, and in the consequent release into the bloodstream of bacterial toxins, resulting in a systemic inflammatory response. This reaction may occur between 1–12 hours after antibiotics are initiated but can also occur later and last for a few hours or up to two days. Symptoms include a worsening of fever, chills, muscle pains and headache. If this occurs, patients are advised to consult their doctor.15, 16, 17
- Resolve psychoemotional trauma and stress associated with the tick-borne illness. Journaling important past traumatic events; meditation; taijiquan (Tai Chi); movement and dance.
- Modulate immunity using medicinal mushrooms, honeybee propolis and immunological herbs.18
- Focus on reducing overall inflammation; may use curcumin and proteolytic enzymes.
- Improve methylation with methyl donors such as methylated B12 and methylated folate.19
- Balance intestinal microbiome with pre- and probiotics; internal bentonite clay helps remove toxic intestinal biofilm.
- Resolve structural misalignments.
- Improve the oral microbiome -resolve dental foci such as root canal treated teeth and cavitations.
The types and duration of treatments vary with the stage and nature of the infection(s) and must be evaluated by a physician on a case-by-case basis.
Co–infections of Lyme Disease
Ticks carry many bacteria, viruses, fungi and protozoans all at the same time and can transmit them in a single bite. Hence, a huge body of research shows that many chronic Lyme patients have co-infections with multiple tick-borne pathogens.20, 21 Microbes exist in communities: bacteria, viruses, mycoplasma, parasites and molds co-habitate. One species supports and mutually benefits from the other. Studies have shown that co-infection results in a more severe clinical presentation, with more organ damage, and the pathogens become more difficult to eradicate.22 It is not uncommon to see 4 or more combinations of infections in chronic Lyme disease patients. The first three organisms of the following list are the most prevalent coinfections and will be briefly discussed.
- Babesia (protozoa)
- Bartonella (bacteria)
- Ehrlichia (rickettsia)
- Mycoplasma (L-form)
- Anaplasma (rickettsia)
- Coxiella (rickettsia)
- Chlamydia (bacteria)
- Viruses (EBV; CMV)
Babesia (Piroplasmosis or Babesiosis)
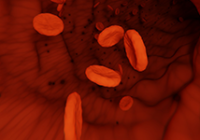
Babesia is a tiny parasite that infects red blood cells. It has been published that as many as 32% of Lyme patients show serologic evidence of co-infection with Babesia microti.23 Babesia infections can range in severity from mild, subclinical infection, to potentially life-threatening illness. Subclinical infection is often missed because the symptoms are incorrectly ascribed to Lyme. Babesia infections, even mild ones, may recur even after treatment and cause severe illness. This phenomenon has been reported to occur at any time, including up to several years after the initial infection. Babesiosis symptomology presents with a more acute initial illness. Patients often recall a high fever and chills at the onset of their Lyme. They also remember night sweats, air hunger, an occasional cough, persistent migraine-like headaches, a vague sense of imbalance without true vertigo, encephalopathy and fatigue.
Diagnostic tests for Babesiosis are insensitive and problematic. Standard blood smears reportedly are reliable for only the first two weeks of infection, thus are not useful for diagnosing later infections and milder ones including carrier states where the parasite load is too low to be detected. It is best to treat based on clinical presentation, even with negative tests.
These parasites are not bacteria, they are protozoans. Therefore, they will not be eradicated by any of the currently used antibiotic Lyme treatment regimens. Therein lies the significance of co-infections – if a Lyme patient has been extensively treated yet is still ill, and especially if they are experiencing atypical symptoms, suspect a co-infection. Treating Babesia is often unsuccessful with Rx therapy. Newer conventional medicine regimens involve a combination of atovaquone (Mepron, Malarone), 750 mg, twice daily, plus an erythromycin-type drug, such as azithromycin (Zithromax), clarithromycin (Biaxin), or telithromycin (Ketek) in standard doses. This combination has resulted in slightly improved success over previous Rx meds; however, atovaquone is very expensive and side effects from these drugs can be severe. Instead, a safe and effective herb treatment for Babesia, like malaria, is Artemisia annula. Specifically, as Artemisinin capsules – 100 mg, 3 times daily for 4 to 6 weeks.
Ehrlichia
The potential transmission of Ehrlichia during tick bites is the main reason why doxycycline is now the first pharmaceutical choice in treating tick bites and early Lyme, before serologies can become positive. When present alone or co-infecting with Lyme, persistent leukopenia (low white count) is an important clue. Thrombocytopenia (low platelets) and elevated liver enzymes, common in acute infection, are less often seen in those who are chronically infected, but likewise should not be ignored. Headaches, myalgias, and ongoing fatigue suggest this illness, but are extremely difficult to separate from symptoms caused by Lyme.24
Testing is problematic with Ehrlichia, like the situation with Babesiosis. More species are known to be present in ticks than can be tested for with clinically available serologies and PCRs. In addition, serologies and PCRs are of unknown sensitivity and specificity. Consider this diagnosis in a Lyme Borreliosis patient not responding well to Lyme therapy who has symptoms suggestive of Ehrlichia.
Standard conventional medicine treatment consists of doxycycline, 200 mg daily, for two to four weeks. A safe and effective herbal remedy for Ehrlichia is the homeopathic (mother tincture) of Colchicum Autumnale (Autumn Crocus) – 20 drops daily for seven days, repeat 10 days if necessary.
Bartonella
Bartonella is a genesis of gram-negative bacteria considered to be the most common of all tick-borne pathogens. It can also be transmitted by other insect vectors such as fleas, sand flies, and lice. There seems to be a distinct clinical syndrome when this type of organism is present in the chronic Lyme patient.25 Early signs of bartonellosis include fever, fatigue, headache, poor appetite, and an unusual streaked rash that resembles “stretch marks” from pregnancy (Bart marks). Swollen glands are typical, especially around the head, neck and arms. Bartonella, like bacterial some other bacterial, can cause abnormal angiogenesis, or the development of microvessels.
The conventional medicine drug of choice to treat Bartonella is the toxic and often problematic levofloxacin. Levofloxacin is usually never used for Lyme or Babesia. Levofloxacin and drugs in this family may cause permanent damage to the connective tissue. It should not be given to those under the age of 18, so other Rx alternatives, such as azithromycin, are used instead in children. A safe triple-herb regime of choice for Bartonella is Polygonum cuspidatum to counteract the angiogenesis actions of the organisms and reduce inflammation, Eupatorium perfoliatum (boneset) to stimulate immune response, and Ceanothus americanus (red root) to clear the lymphatics.
Antibiotic Limitations
The traditional recommended treatment, upon finding an engorged tick and making the clinical diagnosis, is a seven to ten-day regimen of oral doxycycline at 100 mg twice daily for ages greater than eight, excluding pregnant women. This regimen has the advantage of sometimes curing the disease Ehrlichiosis, caused by a gram-negative bacterium carried by Ixodes ticks and a frequent co-infection in endemic areas. Second line Rx therapy includes medications such as amoxicillin and cefuroxime, which patients may be able to order from an online pharmacy similar to a Canadian pharmacy after speaking with their medical physician. However, failures are common with this traditional approach and, in fact, many published studies report less than perfect response rates with doxycycline, amoxicillin, and other oral antibiotic programs. While many patients may appear cured with a 2-4-week antibiotic therapy (symptoms abated), a significant percent of patients continue to suffer persistent symptoms of fatigue, pain or joint and muscle aches, and neurocognitive disorders despite the treatment. This condition is called post-treatment Lyme disease syndrome (PTLDS). The cause for PTLDS is unclear but one strong possibility is persistent infection with Borrelia which is known to develop morphological variant forms such as round bodies (spheroplasts) and aggregated biofilm-like microcolonies.26, 27, 28
Antibiotics do not destroy the mycotoxins or help the body rid itself of the BLP (bacteria lipoprotein neurotoxins) caused by Borrelia. Antibiotics are not effective in treating the various viral, fungal, and parasitic co-infections attendant to Lyme disease. The pharmaceutical challenge of Lyme disease centers on the lack of evidence to support use of antibiotics for longer than 4 weeks.29, 30 There have been several “point and counterpoint” editorials on the benefits and detrimental consequences of long-term antibiotic treatment for Lyme disease. Generally, most studies do not recommend long-term antibiotics for Lyme disease.31, 32 Additionally, the Infectious Disease Society of America and the Center for Disease Control do not recommend prolonged treatment with antibiotics.33
Hence, many individuals develop chronic Lyme because they are solely and ineffectively treated with antibiotic therapy. In these cases, bioregulatory medicine using herbs and other multidisciplinary approaches, offers many advantages in both safety and efficacy.
Diagnosis and Testing
Diagnosing Lyme is often a complicated process and many physicians are not adequately qualified to identify Lyme disease. Additionally, the common tests (Western Blot and ELISA) used to confirm a Lyme diagnosis can report incorrect results 50% of the time.34 In the absence of a defining erythema migrans rash, or “bull’s eye rash”, the clinical symptoms for Borrelia infection are ill defined and ambiguous. In addition, the human antibody response to Borrelia infection develops slowly; this makes early detection challenging for antibody screening tests. First, if you suspect that you have Lyme disease and have not been tested, download and fill out the Horowitz Lyme-MSIDS Questionnaire.35
Physicians typically diagnose and initiate treatment for Lyme disease based on a combination of clinical symptoms and results from laboratory testing, but there are some exceptions. The Center for Disease Control (CDC), International Lyme and Associated Diseases Society, and the Infectious Diseases Society of America have developed guidelines for physicians to follow when diagnosing Lyme borreliosis. The CDC recommends that physicians follow a two-tier testing protocol. The first tier utilizes IgM or IgG-based ELISAs, or IFA, to determine if antibodies from exposure to Lyme Borrelia are present in the patient’s serum. According to the CDC, “if it tests negative, then no further testing is required.” However, also according to the CDC, “the diagnosis of Lyme disease is based primarily on clinical findings, and it is often appropriate to treat patients with early disease solely on the basis of objective signs and known exposure.”
The second tier is another round of immune response testing employing IgM and/or IgG Western blot methods. A Western blot looks for antibodies that are specific to different antigens produced by Borrelia. The CDC criteria for a surveillance case require that an IgM Western blot sample contain antibodies that are reactive to 2 out of 3 antigens to be considered positive. An IgG Western blot requires reactivity to 5 out of 10 antigens for a positive result that meets CDC criteria for surveillance reporting.
“Absence of proof is not proof of absence.”
However, currently, no test can rule out Lyme disease. A person can test negative, but still have Lyme disease. Lyme disease is a clinical diagnosis and testing can support clinical presentation, but not always. Diagnosis of Lyme disease should not be contingent on surveillance criteria which require a positive ELISA followed by five positive CDC bands on a Western Blot. Both the ELISA and Western Blot tests should ideally be conducted to get the most accurate blood testing results possible. Most insurance companies will only pay for one test, so the patient should consider paying out of pocket for the other. When used as part of a diagnostic evaluation for Lyme disease, the Western Blot should be performed by a laboratory that reads and reports all the bands related to Borrelia burgdorferi.
Recommended Laboratory – IGeneX offers several Lyme and coinfection panels. (See Website)36
C6 Lyme Peptide ELISA Test – Oxford Immunotec
C6 Lyme Peptide ELISA test37 is based on the discovery of six (6) peptides on the surface of the spirochete, which are consistently present and do not evade detection by the laboratory as many of the other surface antigens of Borrelia do. This test detects all Borrelia burgdorferi strains and genospecies. It is highly specific and appears more sensitive than conventional tests for chronic Lyme disease. 38 It is also sensitive in early Lyme disease. Like other testing, negative test results should not be used to exclude Lyme disease.
“Treat the patient, not the lab test!”
Summary
Clinicians should be aware of the clinical signs of tick-transmitted diseases, because morbidity can increase substantially if there are delays in diagnosis and treatment. With the incidence of antibiotic failures and the potential of developing post-treatment Lyme disease syndrome, a more comprehensive biological regulatory medicine approach can help speed healing-time, enhance quality of life, and minimize the recurrence of Lyme disease.
For more information on Bioregulatory Medicine and its treatments, visit the Bioregulatory Medicine Institute (BRMI) website at www.brmi.online.
References
- https://www.cdc.gov/lyme/datasurveillance/index.html
- Ogrinc, K., et al., Course and Outcome of Early European Lyme Neuroborreliosis (Bannwarth Syndrome): Clinical and Laboratory Findings. Clinical Infectious Diseases, 2016. 63(3): p. 346-353.
- Middelveen, Marianne, Eva Sapi, Jennie Burke, Katherine Filush, Agustin Franco, Melissa Fesler, and Raphael Stricker. Persistent Borrelia infection in patients with ongoing symptoms of Lyme disease. In Healthcare, vol. 6, no. 2, p. 33. Multidisciplinary Digital Publishing Institute, 2018.
- Wang, Xing-Guo, Joanna P. Scagliotti, and Linden T. Hu. Phospholipid synthesis in Borrelia burgdorferi: BB0249 and BB0721 encode functional phosphatidylcholine synthase and phosphatidylglycerolphosphate synthase proteins. Microbiology150, no. 2 (2004): 391-397.
- Kobryn, Kerri, Darius Z. Naigamwalla, and George Chaconas. Site?specific DNA binding and bending by the Borrelia burgdorferi Hbb protein. Molecular microbiology37, no. 1 (2000): 145-155.
- Mursic, Vera Preac, Sylvia Reinhardt, Bettina Wilske, U. Busch, G. Wanner, and W. Marget. Formation and cultivation ofBorrelia burgdorferi spheroplast-L-form variants. Infection24, no. 3 (1996): 218-226.
- Murgia, Rossella, Chiara Piazzetta, and Marina Cinco. Cystic forms of Borrelia burgdorferi sensu lato: induction, development, and the role of RpoS. Wiener klinische Wochenschrift114, no. 13/14 (2002): 574-579.
- Gruntar, Igor, Tadej Malovrh, Rossella Murgia, and Marina Cinco. Conversion of Borrelia garinii cystic forms to motile spirochetes in vivo Note. Apmis109, no. 5 (2001): 383-388.
- Smith, Aaron J., John Oertle, and Dino Prato. Chronic Lyme disease: persistent clinical symptoms related to immune evasion, antibiotic resistance and various defense mechanisms of Borrelia burgdorferi. Open Journal of Medical Microbiology4, no. 04 (2014): 252.
- Garcia?Monco, Juan Carlos, and Jorge L. Benach. Lyme neuroborreliosis. Annals of Neurology: Official Journal of the American Neurological Association and the Child Neurology Society37, no. 6 (1995): 691-702.
- Lectins are carbohydrate-binding proteins that can bind to cell membranes. For plants lectins are primarily a defense mechanism. Essentially, they are a low-level toxin. The purpose of lectins in plants is to discourage other animals from eating that plant or life form. By triggering a negative reaction in the predator, that life form is then viewed as an undesirable food source, thus, aiding its future survival. In short, lectins can interact with surface antigens found on the body’s cells, causing them to agglutinate or stick together. Hence, lectins are considered another major family of protein antinutrients. Lectins are like antibodies in their ability to agglutinate red blood cells. Essentially, they can cause inflammation in the body.
- Dietrich Klinghardt, M. D. BIOTOXINS – http://klinghardtinstitute.com/wp-content/uploads/2015/06/1.-Biotoxin-chapter.pdf
- Dietrich Klinghardt, M. D. Chronic Illness: the hidden causes. – https://aonm.org/wp-content/uploads/2018/01/Dr.-Dietrich-Klinghardt-AONM-15-Nov-2015-presentation-part1.pdf
- For HPU diagnosis with urine analysis for Kryptopyrrol, suggest using The Great Plains Laboratory, Inc. 11813 W. 77th St.; Lenexa, KS 66214 USA 800-288-0383.
- Belum, Geetanjali Reddy, Viswanath Reddy Belum, Sri Krishna Chaitanya Arudra, and B. S. N. Reddy. The jarisch–herxheimer reaction: Revisited. Travel medicine and infectious disease11, no. 4 (2013): 231-237.
- Maloy, Anna L., Robert D. Black, and Romualdo J. Segurola Jr. Lyme disease complicated by the Jarisch-Herxheimer reaction. The Journal of emergency medicine16, no. 3 (1998): 437-438.
- Moore, J. A. Jarisch-Herxheimer reaction in Lyme disease. Cutis39, no. 5 (1987): 397-398.
- Stamets, Paul Edward. Antiviral and antibacterial activity from medicinal mushrooms. U.S. Patent 8,765,138 issued July 1, 2014.
- Your DNA consists of four bases, called cytosine, guanine, adenine, and thymine. A chemical unit called a methyl group, which contains one carbon and three hydrogen atoms, can be added to cytosine. When this happens, that area of the DNA is ‘methylated’. When you lose that methyl group, the area becomes demethylated. DNA methylation often inhibits the expression of certain genes. For example, the methylation process might stop a tumor-causing gene from “turning on,” preventing cancer. Methyl groups are important for numerous cellular functions such as DNA methylation, phosphatidylcholine synthesis, and protein synthesis. The methyl group can directly be delivered by dietary methyl donors, including methionine, folate (folic acid), methylated B-12, betaine, and choline. Some individuals with Lyme disease lack methyl donors, and thus, have problems with methylation.
- Moutailler, Sara, Claire Valiente Moro, Elise Vaumourin, Lorraine Michelet, Florence Hélène Tran, Elodie Devillers, Jean-François Cosson et al. Co-infection of ticks: the rule rather than the exception. PLoS neglected tropical diseases10, no. 3 (2016): e0004539.
- Horowitz, Richard, Allen Richards, Megan Dulaney, Marna E. Ericson, Christine Green, Charles Lubelczyk, Ulrike Munderloh et al. Other Tick-Borne Diseases and Co-Infections. (2018).
- Wormser, Gary P., Donna McKenna, Carol Scavarda, Denise Cooper, Marc Y. El Khoury, John Nowakowski, Praveen Sudhindra et al. Co-infections in Persons with Early Lyme Disease, New York, USA. Emerging Infectious Diseases25, no. 4 (2019): 748.
- Djokic, Vitomir, LAVOISIER AKOOLO, Shekerah Primus, Samantha Schlachter, Kathleen Kelly, Purnima Bhanot, and Nikhat Parveen. Protozoan parasite Babesia microti subverts adaptive immunity and enhances Lyme disease severity. Frontiers in Microbiology10 (2019): 1596.
- Dumler, J. Stephen, and Johan S. Bakken. Ehrlichial diseases of humans: emerging tick-borne infections. Clinical infectious diseases20, no. 5 (1995): 1102-1110.
- Higgins, R. Emerging or re-emerging bacterial zoonotic diseases: bartonellosis, leptospirosis, Lyme borreliosis, Revue Scientifique et Technique-Office International des Epizooties 23, no. 2 (2004): 569-582.
- Feng, Jie, Tingting Li, Yuting Yuan, Rebecca Yee, and Ying Zhang. Biofilm/Persister/Stationary Phase Bacteria Cause More Severe Disease Than Log Phase Bacteria I Biofilm Borrelia burgdorferi Not Only Display More Tolerance to Lyme Antibiotics but Also Cause More Severe Pathology in a Mouse Arthritis Model: Implications for Understanding Persistence, PTLDS and Treatment Failure. bioRxiv(2018): 440461.
- Feng, Jie, and Ying Zhang. Proteomic Analyses of Morphological Variants of Borrelia burgdorferi Shed New Light on Persistence Mechanisms: Implications for Pathogenesis, Diagnosis and Treatment. bioRxiv(2018): 501080.
- Rudenko, Natalie, Maryna Golovchenko, Katerina Kybicova, and Marie Vancova. Metamorphoses of Lyme disease spirochetes: phenomenon of Borrelia persisters. Parasites & vectors12, no. 1 (2019): 237.
- Borchers AT, Keen CL, Huntley AC, Gershwin ME. Lyme disease: A rigorous review of diagnostic criteria and treatment. J. Autoimmun 2015;57:82– 115.
- Rowe PM. Chronic Lyme disease: the debate goes on. Lancet 2000;355:1436.
- Shaw, Gina. Prolonged Antibiotics Do Not Improve Neurocognitive Outcomes in Persistent Lyme Disease. Neurology Today19, no. 5 (2019): 27-31.
- Auwaerter, Paul G. Point: antibiotic therapy is not the answer for patients with persisting symptoms attributable to lyme disease. Clinical Infectious Diseases45, no. 2 (2007): 143-148.
- Wormser GP, Nadelman RB, Dattwyler RJ et al. Practice guidelines for the treatment of Lyme disease. The Infectious Diseases Society of America. Infect. Dis. 31(Suppl. 1), 1–14 (2000).
- Lin Zhang, X.Z., Xuexia Hou, Zhen Geng, Hai Chen, and Qin Hao1, Test of 259 serums from patients with arthritis or neurological symptoms confirmed existence of Lyme disease in Hainan province, China. 2015, US National Library of Medicine.
- http://lymeontario.com/wp-content/uploads/2015/03/Horowitz-Questionnaire.pdfigenex.com -797 San Antonio Rd., Palo Alto CA 800.832.3200.
- C6 Lyme Peptide ELISA test (Boston Biomedica Inc DBA – BBI Clinical Laboratories, 75 N Mountain Rd, New Britain, CT,06053 Tel.: 1-800-676-1881 or 1-508-580-1900, test code: 556 – C6LPE).
- Tjernberg, Ivar, G. Krüger, and Ingvar Eliasson. C6 peptide ELISA test in the serodiagnosis of Lyme borreliosis in Sweden. European Journal of Clinical Microbiology & Infectious Diseases26, no. 1 (2007): 37-42.
- Jansson, C., S-A. Carlsson, H. Granlund, P. Wahlberg, and D. Nyman. Analysis of Borrelia burgdorferi IgG antibodies with a combination of IgG ELISA and VlsE C6 peptide ELISA. Clinical microbiology and infection11, no. 2 (2005): 147-150.
Additional Resources and References
Books and Articles
- Burrascano, Joseph J. , MD, Advanced Topics in Lyme Disease Diagnostic Hints and Treatment Guidelines for Lyme and Other Tick-Borne Illnesses; Sixteenth Edition Copyright October, 2008 – http://www.lymenet.org/BurrGuide200810.pdf
- Buhner, Stephen Harrod.: Healing Lyme: Natural Prevention and Treatment of Lyme Borreliosis and Its Coinfections
- Newby, Kris: Bitten – The Secret History of Lyme Disease and Biological Weapons
- Horowitz, Richard – How Can I Get Better? An Action Plan for Treating Resistant Lyme and Chronic Disease
- Horowitz, Richard – Herbs, Hormones & Heavy Metals: A study of CAM therapies in the Treatment of Chronic Lyme Disease
- Singleton, Kenneth B – The Lyme Disease Solution
- Weintraub, Pamela – Cure Unknown: Inside the Lyme Epidemic
Laboratories
Supplement Companies
- Biopure – https://biopureus.com/
- Rainforest Pharmacy – https://myherbs.net/rainforest-pharmacy/
- Bio Essence https://bioessence.com/search?type=product&q=mushrooms
- SunTen Herbs – https://www.sunten.com/
Websites
- International Lyme and Associated Diseases Society (ILADS) –ILADS.org Guidelines – https://www.tandfonline.com/doi/full/10.1586/14787210.2014.940900
- lymeinfo.net
- klinghardtacademy.org
- brmi.online
ADDENDUM 1 – Overview of Lyme Borreliosis (A Bioregulatory Medicine Approach)
Basic Principles:
- Decrease Pathogenic Microbial Load (Plant-based Antimicrobials, IV Ozone, Rizols)
- Improve Intestinal and Oral Microbiome
- Decrease Total Toxic Body Burden
- Balance and Modulate the Immune System
- Improve Bioregulatory Mechanisms (Heme Synthesis, Methylation)
There are several herbs that have been clinically used to decrease pathogenic microbial load and treat Lyme and its co-infections. Some are used solo, some work better in combination, and there are many formulations available as well. This, as all therapy, needs to be individually assess as to which ones are appropriate, dosage, timing and herbal alterations or rotations. The following are some of the most commonly employed.
Artemisia annua (Sweet Wormwood; Qing Hao ??)
Bitter Flavor; cold property; liver and gallbladder meridians
Actions:
- Antibacterial effect
- Anti-malarial
- Anti-parasitical
- Psycho-emotional Signature: Mental Clarification
Long been used in TCM for malaria; useful in treatment of Babesia co-infection; treating Babesia first will promote better outcome in the treatment of Lyme disease; can help reducing Herxheimer reaction; important to also stimulate lymphatics and support the spleen.
Artemisia annua Dosage: babesia or malaria – 100 mg 2 – 3x daily for two weeks, repeated again in one week with grapefruit juice; 2 weeks on, 1 week off; (30 to 60 days, some difficult cases may take 6 months to 1 year treatment for Babesia) Sources: Biopure – Artemisinin – powder – standardized extract, 24 grams, comes with spoon; serving is 1 scoop – 100 mg 2 x daily. At regular servings this equals 60 total servings per bottle.
Allergy Research – 30:1 500 mg 100 capsules – 100mg 2 x daily
Andrographis paniculata (Chuan Xin Lian ???)
Bitter Flavor “King of Bitters”; cold property; lung, stomach, large intestine and bladder meridians
Common Usage: prophylaxis and symptomatic treatment of upper respiratory infections, such as the common cold and uncomplicated sinusitis, bronchitis and tonsillitis, lower urinary tract infections and acute diarrhea.
Actions:
- Immune modulator
- Anti-inflammatory
- Protects and supports liver function
- Protects CNS
- Eliminates intestinal infestations
- Historically, used to treat syphilis – it’s claimed to be anti-spirochetal
Andrographis paniculata: Contains: diterpene lactones known as andrographolides – andrographolide, deoxyandrographolide, neoandrographolide, 5,7, tetramethoxyflavanone and 5-hydroxy-7, trimethoxyflavone, as well as several other flavonoids and polyphenols.
Often combined with other herbs in treatment of Lyme disease.
Andrographis Initial dosage: 400 capsule 3x daily; gradually increase one capsule every 7 days till dosage is 3 capsules 1200mg 4x daily; after symptoms subside reduce slowly.
Available: Standardized 10% andrographolides
Smilax glabra (Sarsaparilla) Tu Fu Ling ???
Sweet bland flavor; neutral property
Sarsaparilla contains: sarsasapogenin, smilagenin, sitosterol, stigmasterol, and pollinastanol; and the saponins sarsasaponin, smilasaponin, sarsaparilloside, and sitosterol glucoside, among others.
Sarsaparilla Properties/Actions:
Anti-inflammatory, anti-spirochetal; antibacterial, antifungal, blood cleanser, detoxifier, diuretic, hepatoprotective, protects brain cells, blood cleanser, immunomodulator, antimutagenic, detoxifier, tonic (tones, balances, strengthens overall body functions)
Sarsaparilla has long been used in China for the treatment of syphilis. Clinical observations in China demonstrated that sarsaparilla was effective in treatment of syphilis (according to blood tests) in about 90% of acute and 50% of chronic cases. Useful as anti-Herxheimer reaction, with unresolved brain fog, confusion, weakness.
Sarsaparilla Source and Dosage: Biopure tincture – available in 2 fluid oz. 1 drop per day for 4 days, doubling the dose every 4 days until the full dose of 16 drops per day is reached. If side effects are experienced, reduce to the last tolerable dose.
Polygonum cuspidatum (Japanese Knotweed) Hu Zhang ??
Traditional Chinese medicine properties are sour, bitter, mildly pungent flavor; cold; enters liver, gallbladder and lung meridians; used traditionally in China for supporting the body’s natural detoxification pathways, to clear blood of toxic heat and eliminate blood stasis, as a cardiac tonic, mild laxative and as a diuretic. Tonics have been used throughout history for a range of medical purposes – you can read the history of different medicines here.
Roots of P. cuspidatum contain compounds called stilbenes; one stilbene called resveratrol has several physiological activities. Primarily, the root inhibits the growth of several bacteria and fungi (Kubo, et al, 1981) – including leptospira and Treponema denticola spirochetes. It is anti-inflammatory and helps reduce Herxheimer reactions.
Japanese Knotweed Actions:
Its antimicrobial activity is not only due to resveratrol, but to 2-methoxy-6-acetyl-7-methyljuglone, a naphthoquinone (Kimura, et al, 1983a; Yamaki, et al, 1988). It protects against endotoxin damage and is a cardioprotector. Its constituents cross the blood-brain barrier and protects against oxidative damage and microbial endotoxins.
Japanese Knotweed Sources and Dosage:
Tincture (Biopure): 1 drop per day for 4 days, doubling the dose every 4 days until the full dose of 16 drops per day is reached. If side effects are experienced, go back to the last tolerable dose. Put drops in 1 – 2oz of filtered, organic apple juice to hide the bitter taste.
Tablets (Source Naturals, Resveratrol Antioxidant Protection 40mg) 1 – 4 tablets 3-4 x daily beginning at lowest dose increasing every seven days. Maintain two months then lower to maintenance dose 8 to 12 months.
Quintessence Formula by Biopure
Quintessence: Quintessence is a combination of five herbal tinctures that work together, creating a potent broad-spectrum approach to immune system support. Contains organic tinctures of Andrographis, Smilax, Stephania Root, Japanese Knotweed and Red Root.
Source: Biopure – Dosage: The average adult may take up to 8 droppers full of Quintessence diluted in 1 liter of water and drunk throughout the day.
Coptis chinensis (Huang Lian ??)
Root exhibits bitter flavor, cold property; disperses heat, dries dampness, purges fire, removes toxin; enters the heart, liver, gall bladder stomach and large intestine meridians
Coptis chinensis actions: Anti-inflammatory, antibacterial, antifungal, antiviral (influenza viruses), vasodilator, anti-pyretic, anti-diarrhea, cholagogue, anti-ulcer, stomachic, anti-protozoal, immune stimulant. Coptis is a choleretic shown to triple bile secretion for 1.5 hours
Coptis chinensis contains: Alkaloids: Berberine (7-9%), coptisine, atrorrhizine, palmatine, epiberberine, jatrorrhizine, urbenine, worenine, palmaline,, columbamine. Berberine and berberine-like alkaloids are primarily responsible for its antimicrobial activity.
Clinically, berberine has been used to treat giardia, cholera, amebiasis, as well as visceral and cutaneous leishmaniasis. It strongly inhibits Streptococcus pneumoniae, Neisseria meningitis, and Staphylococcus aureus.
Dosage: Coptis Tea Pills (Plum Flower Brand) 4-8, 3-4X daily Source: Mayway Trading
Eight (8) Traditional Chinese Herbs for Lyme disease:
- Andrographis paniculata (Chuan Xin Lian) – anti-spirochetal, antimicrobial, immune stimulant, anti-inflammatory, enhances liver function
- Coptis chinensis (Huang Lian) Antitoxin heat clearing; strong antimicrobial
- Scutellaria barbata (Ban Zhi Lian) Antitoxin heat clearing
- Artemesia annua (Qing Hao) – Anti-parasitic
- Smilax glabra (Tu Fu Ling) – Lymphatic cleanser, anti-spirochetal, anti-Herxheimer reaction
- Flos Lonicerae japonicae (Jin Yin Hua) Antitoxin heat clearing
- Fructus Forsythiae (Lian Qiao) Antitoxin heat clearing
- Isatis root (Ban Lan Gen); Isatis leaf (Da Qing Ye) – Anti-toxin heat clearing
Traditional Chinese Medicine Formula for Lyme disease:
- Huang Lian Jie Du Tang (Sun Ten Brand) – Coptis Scute Combination – 100 Sun Ten Capsules – General Dose 1-2 capsules 2-3 times per day. At full dose lasts approximately 16 days.
David Winston’s Spirolyd Compound
Specific for spirochetes
Contains Extracts of sarsapilla root, andrographis herb, guauacum wood, prickly ash bark, stillingia root.
Dosage 40-60 drops (2-4 mL) in juice or water. Take 3 times per day. Shake well before using.
Rain Forrest Herbs and Formulas
Uncaria tomentosa; Uncaria guianensis (Cat’s Claw – uña de gato)
Both South American Uncaria species are used by the indigenous peoples of the Amazon rainforest in very similar ways and have long histories of usage (2000 years) – for treating gastrointestinal and infectious diseases.
Usages: all inflammatory conditions, immunological disorders, cancer and Lyme.
Cat’s Claw Chemical Properties:
- Oxidole alkaloids – documented with immune-stimulant and antileukemic properties.
- Carboxyl alkyl esters – immunostimulant, anti-inflammatory, anti-cancerous properties.
- Quinovic acid glycosides -anti-inflammatory and antimicrobial actions.
- Antioxidant chemicals – tannins, catechins and procyanidins
- Plant sterols – beta-sitosterol, stigmasterol, campesterol exhibit anti-inflammatory properties.
Cat’s Claw Dosage: The best source of cat’s claw extract contains 3% total alkaloids. For general immune and prevention benefits – 1 g daily of vine powder in tablets or capsules. Therapeutic dosages of cat’s claw are from 5 to 20 g daily and average 2-3 grams two or three times daily. Supplementing with probiotics and digestive enzymes is advisable if Cat’s Claw is used for longer than 15 days.
Brosimum acutifolium (Tamamuri)
Tamamuri is a large canopy tree of the Amazon; grows 15 to 25 m and produces light pink latex when the smooth trunk bark is wounded, or the leaf stems are broken from the branches. Tamamuri is found throughout lower elevations usually growing alongside streams and rivers where its fruits are eaten by fish when they fall from the tree.
Tamamuri bark contains: flavans, flavanoids, lignans, phenylpropanoids, benezoids, and steroids. Many of these chemicals are novel ones never before discovered by scientists, including 6 chemicals they’ve named acutifolins and 13 chemicals they’ve named brosimacutins.
Tamamuri Actions:
- Antiinflammatory – In traditional medicine the bark is used as an anti-inflammatory and a treatment for rheumatism. Tamamuri’s long-standing use for arthritis and rheumatism has been the subject of research by Western scientists.
- Anti-spirochete – It is both effective for Lyme and syphilis.
Tamamuri Dosage: As tincture: 60 drops 2 – 3 X daily; this plant is best prepared as a decoction. Use one teaspoon of powder for each cup of water. Bring to a boil and gently boil in a covered pot for 20 minutes. Allow to cool and settle for 10 minutes and strain warm liquid into a cup (leaving the settled powder in the bottom of the pan). It is traditionally taken in 1 cup dosages 3 times daily
Rainforest Amazon Spiro – Contains Six Herbal Ingredients:
- Chanca piedra whole herb (Phyllanthus niruri)
- Bellaco caspi bark (Himatanthus sucuuba)
- Tamamuri bark (Brosimum acutifolium)
- Matico leaf (Piper aduncum)
- Huacapu bark (Minquartia guianensis)
- Ajos sacha bark & leaf (Mansoa alliacea).
Rizols
Rizols (as produced by Biopure) are ozonated castor oil remedies treated with high voltage electrolysis with added plant oils designed when taken orally to decrease microbial count. Rizols have strong and specific anti-microbial properties, are relatively easy and pleasant to take.
Different Rizols:
- Gamma Rizol contains: Oil of Artemisia, Clove Oil, Walnut Oil.
- Zeta Rizol contains: Oil of Artemisia, Clove Oil, Black Cumin Oil, Moxa Oil, Walnut Oil
- Epsilon Rizol contains: Oil of Artemisia, Clove Oil, Black Cumin Oil, Walnut Oil, Garlic Oil, Marjoram Oil
- Kappa Rizol contains: Oil of Artemisia, Clove Oil, Black Cumin Oil, Walnut Oil Thyme Oil, Marjoram Oil
Rizols may be taken orally in two ways:
- One or more drops may be dropped in an empty glass. Then good quality water is poured from a height so that the oil and water create half a glass of whitish emulsion. This may be taken on an empty stomach.
- Alternatively, empty capsules may be filled with one or more drops of rizol, closed and swallowed with a glass of water.
Rizol Dosage – Practitioners may recommend adults building up from 1 drop to 15-20 drops of Rizol, 3 times per day for several months. Energetic testing to determine which rizol to start – usually Gamma and/or Zeta; Start slow, build up to full dose over 2-3 months. After 2-3 months test again – replace Zeta with Epsilon. Start slow!
Related Posts